

Libido through the Lifespan
The Biology, Psychology and Culture of Sex Drive


One of the many upshots of being a solo-polyamorous person is that I’m not responsible for maintenance sex. I have mind-altering, creative, powerful sex when and with whom I want. If I’m not feeling playful, I don’t have to engage. My lack of libido isn’t holding anyone else’s sexual life hostage. Which is a good thing considering how much my libido has tanked over the last 6 weeks. For reasons related to national security…
It’s okay to not want sex. If you’re not bothered by not having sex, there’s no problem. Lack of libido or libido mismatch IS a problem in the context of a sexually exclusive, monogamous relationship and is a common cause of marital discord and infidelity. It can be a big problem if one partner feels as though they’ve been sexually abandoned or if one partner feels like they’re being badgered for sex that they don’t want to have.
From my perspective, a vow of monogamy is not meant to be a vow of celibacy. I also believe that sexless, companionate marriages are completely valid if both partners consent to maintaining them. I do believe, however, that allowances need to be made if one partner withdraws entirely from sex on a permanent basis. It’s important to keep in mind, however, that postpartum, medical conditions and transient high-stress professional circumstances are NOT permanent. In these cases, patience and compassion are vital.
Given the complete lack of sexual health education in the United States, no one is equipped to talk about how libido impacts relationships. Thus, we have a culture that uses sex as a barometer for the health of relationships without accounting for the myriad of biological, psychological and social factors that can affect libido. This is a big topic so I’ve broken things down into a few key areas to be rolled out over two weeks. Consider it a warm holiday gift from me to you.
Part One:
A Quick and Dirty Guide to Hormones
The Untold Story of Childbirth and Libido
Aging, Peri/Menopause and a Primer on Hormone Therapy
Part Two:
Medications and recreational drugs
The Role of Novelty and Eroticism
Thanks to everyone in my Substack community who submitted questions! If you hav additional libido-related questions, feel free to drop them in the comments.
You can find my videos on Male and Female Anatomy as well as Pelvic Floor Health at the newly redesigned Under the White Coat page on Substack. In those videos, I cover things like clitoral anatomy, blood flow, Viagra, prostate health/play and testosterone injections.

I’m planning a new video specifically dedicated to Menopause Hormone Therapy. These videos summarize years of medical training and are available exclusively to my paid subscribers. I invite you to join me for an in-depth exploration of the science of human sexuality that you’re probably not getting in your doctor’s office.
***Of note, when I refer to male and female, men and women, I am referring to the anatomy that folks are born with. I recognize and have taken care of trans, non-binary and intersex individuals. The lessons here should apply regardless of gender or sexual orientation.***
On to the Good Stuff…
Another term for libido is sex drive. Influenced by hormones, medical conditions, drugs, stress, psychological and social factors, it’s normal for libido to fluctuate throughout the lifespan. When examining the reasons for decreased romance, it’s important to distinguish between low libido and disinterest in what’s on offer. Desire is a strong feeling of wanting or wishing for something to happen. In order to desire sex, the experience being offered needs to be worthy of desire.
Let’s consider for a moment sex as a form of physical hunger.
One may be hungry and find the idea of food desirable but if all that’s being offered is mushy broccoli, one may prefer to go hungry. The same principal applies to lazy lovemaking. If you want to have better and more frequent encounters, it’s important to be a knowledgeable, communicative and generous lover.
A Quick and Dirty Guide to Hormones
Think of hormones as chemical messengers relaying information throughout the body. Hormones are produced in the brain, the adrenal glands, the gonads (ovaries and testes) and several other tissues.
There are receptors for these chemical messengers all over the place. Signals sent to the heart, brain, gut, bones, skin and muscles can impact our general health, emotional state and sexual function.

Estrogen: receptors in both men and women receive chemical messages relayed by this hormone. Yes, fellas, your body also produces and uses estrogen.
In women, a natural decline of estrogen production occurs after childbirth, during menopause, after surgical removal of one or both ovaries or during chemotherapy. This decline can have widespread effects on nearly every physiological function. Estrogen deficiency can cause emotional distress, decline in cognitive function, decreased muscle mass, loss of bone mineral density, decreased vaginal lubrication and impaired blood flow to the vulva. These symptoms can be quite distressing and contribute significantly to decreased libido.
Progesterone: produced throughout the lifespan but especially by the placenta during pregnancy. Progesterone-only birth control is available for those who can’t take estrogen for medical reasons (ie: people who smoke, have a history of blood clots and those who have migraines with aura). Women who are on estrogen replacement during menopause require progesterone to protect the uterus from the hypertrophic effect of estrogen on uterine tissue.
Prolactin: produced primarily in the pituitary gland by both men and women, this hormone takes center-stage during breastfeeding. As the name implies, prolactin contributes to lactation (milk production) and suppresses the production of estrogen and progesterone. Certain drugs and medical conditions can also increase production of prolactin
Testosterone: wrongly described as the “male sex hormone”. Although men produce more testosterone than women, women produce more testosterone in their own bodies than they do estrogen. Testosterone is a key driver in the maintenance of muscle mass and contributes to energy, exercise tolerance and libido. There are testosterone receptors in the vagina so it also contributes to the maintenance of vaginal health, lubrication and blood flow.
Testosterone is a controlled substance in the US because of the Olympic doping scandals of the 1980’s. Although med spas dole out T to men as a “biohack” for everything from low libido to erectile dysfunction, there is no FDA approved testosterone formulation for women. It’s sometimes prescribed for off-label use in women who have “low libido” but its therapeutic benefits extend far beyond that.
Oxytocin: bonding hormone; produced during sex, cuddling, breastfeeding, labor and emotional bonding.
Pitocin, a pharmaceutical product given to induce labor, mimics oxytocin and causes uterine contractions. The release of oxytocin during breastfeeding can also cause uterine contractions/cramping; a point that I make to new mothers in the early days of breastfeeding.
Cortisol: produced by the adrenal glands all the time but elevated during fight-or-flight responses. Cortisol is a stress hormone; it can suppress libido in times of acute or chronic stress. Including stress related to national security.

The Untold Story of Childbirth and Libido
Whenever a family approaches me during pregnancy about being their baby’s pediatrician, I remind them to enjoy the last few weeks of the pregnancy with some intimate bonding. People understandably get excited for the arrival of the newborn but are often unprepared for the lack of intimacy that commonly comes in the wake of childbirth. There are a variety of reasons for this.
After delivery, OBGYNs recommend avoiding penetrative sex for 6 weeks. This timeline is completely arbitrary and based on the more generalized timeframe for wound healing. Depending on the method of delivery, the mother’s body may have suffered vaginal, urethral or rectal tearing; extensive muscle stretching or even postpartum hemorrhage. Many think of c-section as a routine operation but it’s a major abdominal surgery; one that requires weeks to months of recovery in order to return to a stable baseline.
Many women struggle with incontinence, constipation, hemorrhoids, muscle laxity or muscle hypertonicity after childbirth. Incontinence is the second leading cause for low libido behind depression. And it may take far longer than 6 weeks for these wounds to heal. I recommend pelvic floor PT to everyone both before and after delivery.
Another physiologic change that happens postpartum is that estrogen and progesterone levels plummet. This low-estrogen state can mimic perimenopause; causing symptoms such as low energy, depressed mood, poor sleep, sweats, vaginal dryness and, you guessed it, decreased libido. Prolactin production during breastfeeding suppresses ovulation and menstruation but can also manifest as lack of interest in sex.
Many couples report exhaustion in the first 2-3 months of a baby’s life. Round-the- clock feedings and the adjustment to caring for a newborn can put a huge damper on intimacy. Some women report that they feel “touched out” by constantly having the hands, bodies and mouths of small children on them. Children with special medical needs increase the demands on new parents. Some women also report discomfort with the idea of their breasts being eroticized by their partner when they are a source of nutrition for a new infant. All of these factors can cause a transient (not permanent) decrease in libido. Importantly, these things have nothing to do with the desirability of the partner and are likely to resolve with time, patience and teamwork in parenting tasks.
The reason I recommend that couples enjoy sex during pregnancy is because they may face a prolonged dry spell when they become parents. Honestly, I think that doctors should do a better job of preparing couples for this chapter in their lives.

Aging, Peri/Menopause and a Primer on Hormone Therapy
Bazillions of dollars have been spent to ensure that men can maintain both libido and sexual function well into their golden years. But the medical and scientific communities have barely paid lip service to the preservation of women’s sexual health until the last 10 or so years. Fortunately, thanks to a new generation of physicians and scientists, many of whom are women, the focus is beginning to shift.
Older women often experience discomfort with sex as the result of a condition called Genito-Urinary Syndrome of Menopause (GSM). This condition used to be called vulvovaginal atrophy because it’s essentially a shrinking and drying out of the vulva and vagina.
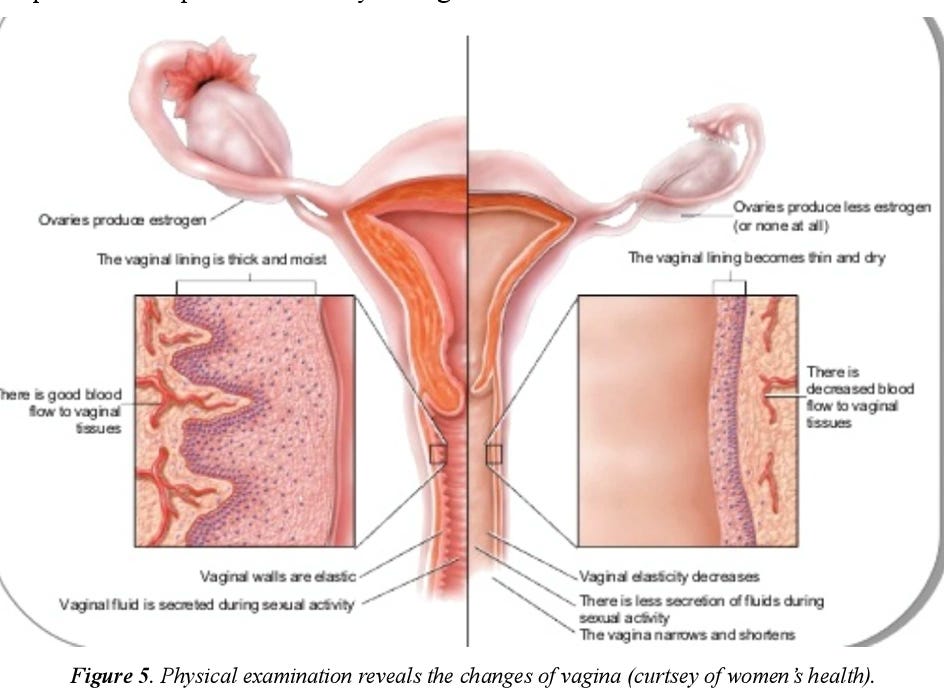
The vulva (external genitalia) and vagina (internal genitalia) need estrogen and testosterone to maintain healthy cellular turnover and blood flow. In the absence of these hormones, the lining of the vagina becomes thin, dry and atrophic (shrunken). Hormone deficiency can also result in atrophy of clitoral tissue due to decreased blood flow. (The female clitoris requires blood flow for engorgement just like the male penis does. Check out my anatomy lessons for a more comprehensive explanation.)
As you can imagine, if one’s vagina is shrunken, dry and unable to experience self-lubrication, elasticity or clitoral engorgement, the pleasure of penetrative sex would dramatically decrease. If you’re a guy, imagine shoving a cucumber into your irritated, un-lubricated anus. Not fun.
These vulvar and vaginal changes are in addition to the systemic changes of the low-estrogen state that I spelled out above. Add in hot flashes, night sweats, brain fog, weight gain, decreased stamina, depression and the stress of caretaking and you can see why women of a certain age may be uninterested in sex.
So what do we do about all of this?
It’s important to ascertain whether decreased libido is the result of relationship problems, poor quality of sex or if the root of the problem is physiologic. Medications and hormone therapy won’t fix bad sex or a broken relationship.
If the problem is hormonal, there are a variety of therapies available including patches, pellets, creams, pills and injections to treat the symptoms associated with postpartum, aging and peri/menopause. Physical therapy and mental health support can also provide remarkable benefits. A complete pharmacologic breakdown is beyond the scope of this piece but I encourage interested readers to contact a clinician that’s certified by The Menopause Society to address treatment of peri/menopause.
Whatever your gender, I believe that adults deserve healthy, nourishing and pleasurable sex throughout the lifespan. Certain seasons of life require patience and self-pleasure. All seasons require communication, generosity as a lover and willingness to be honest with one’s partner.
Next week, I’ll dive into the topics of eroticism, novelty and how drugs can affect libido. Stay tuned!
Resources
If you’re a clinician who wants to expand your understanding of menopause and hormone therapy, I STRONGLY recommend the courses offered by Heather Hirsch Academy. The Menopause Society also has fantastic resources for clinicians.
The International Society for the Study of Women’s Sexual Health and the International Society of Sexual Medicine are doing phenomenal research and teaching on the science of sexual health.
Gratitude for your writing and sharing important information about our bodies and health.
Loved it! Indeed there is not enough talks about healthy sexual life for women after menopause.
I have just discovered last night during a spell of insomnia (another issue accompanying menopause, which deeply affects the energy level and productivity during the day, and which is not talked much about) that my interest in looking feminine decreased as well, as I don't want men eyes on me. My brain offered me the thought that when libido is low, one should not attract any attention.
What a weird thought! Anyone else thinking the same?
Looking forward to read more!